Hodgkinlymfoom (HL)
Inhoudsopgave
Terug naar overzicht hematologische diagnosen http://de-heer.eu
1 Verplicht onderzoek
- PET-CT (geen zekerheid hoog-stadium: in stralingshouding)
- geen beenmergonderzoek
- Ann-Arbor-classificatie
- vroeg-stadium:
- consult radiotherapie voor start chemotherapie
- GHSG-risicoclassificatie
- EORTC-risicoclassificatie
- overweeg ook bij vroeg stadium vruchtbare vrouw te verwijzen naar de fertiliteitpoli
- semenpreservatie
2 Therapie
2.1 therapie eerste lijn
2.1.1 vroeg stadium
- let op: stadium II-B en bulky is gevorderd HL
+--------------------------------+ +------------------------+ | | | | | ›70 (of ›60 en niet fit)? |----->| 3x CHOP-21 + IN-RT | | | | | +------------+-------------------+ +------------------------+ | | | v +------------------------+ +------------------------+ | | | | | argumenten tegen RT? |------>| 4-6x ABVD | | | | | +----------------+-------+ +------------------------+ | | | v +-----------------------------+ | | | 2 -4x ABVD + IN-RT | | | +-----------------------------+ --
- >70 of >60 en niet fit: 3x CHOP-21 + IN-RT
- altijd multidisciplinair bespreken wat betreft wel geen RT
- interim-PET na 2 kuren ABVD: indien D4+ ipv 2x AVD over op 2x escBEACOPP
- 60-70 en fit: als <60 maar zonder escBEACOPP
- na 2 kuren ABVD mag de bleomycine weggelaten worden indien de ABVD gecontinueerd wordt
- daarna therapie eindevaluatie als bij gevorderd
- in principe schema met radiotherapie
- EORTC/GHSG favourable: 2x ABVD + 20 Gy INRT
- GHSG unfavourable
- EORTC favourable: 3x A(B)VD + 20 Gy INRT
- EORTC unfavourable: 4x A(B)VD + 30 Gy INRT
- infradiafragmaal is geen reden om af te wijken van protocol1
- zonder radiotherapie
- therapie zonder RT gering inferieur m.b.t. Hodgkinlymfoom
- indicatie:
- <35 jaar en mammae in veld: mediastinaal en bilateraal axillair
- bij twijfel: proefplanning te overwegen
- bulky mediastinaal, mediastinaal en 1 klier in oksel
- proximaal in hals
- non-bulky: 4x A(B)VD
- bulky: 6x A(B)VD
2.1.2 gevorderd
- keuze tussen start met ABVD of BEACOPP
- >60: altijd ABVD
- argumenten voor escBEACOPP: stadium IV, hoge tumorload (tumor >7 cm), IPS >1, voorkeur patient
- argumenten voor ABVD: fertiliteit, PS >2 boven 40 of co-morbiditeit
- bij begin met ABVD
- 2x ABVD
- PET-CT
- D1-3: nog 4x AVD
- D4-5: 4x escBEACOPP
- begin met escBEACOPP
- 2x escBEACOPP
- PET-CT
- D1-3: 2x escBEACOPP
- D4-5: 4x escBEACOPP
- >70 of >60 en niet fit: 6x CHOP-21
- eindevaluatie
- in bestralingspositie bij grote kans op aanvullende radiotherapie
- na chemoradiotherapie
- na 3 maanden
- niet nodig bij beperkt stadium en negatieve interim/plannings-PET-CT
- na behandelplan zonder radiotherapie
- na 4-6 weken
- indien nieuwe lesies of groei na eerdere afname, en <65 tot 70
- PA-bevestiging: tweedelijns therapie
- geen PA-bevestiging mogelijk: na 2 maanden PET-CT herhalen
- indien "nog resterende FDG-avide afwijkingen" >1,5 cm: aanvullende RT, 36 Gy op FDG-avide afwijkingen
2.2 recidief
- curatieve intentie
- <65-70 en fit genoeg voor autologe stamceltransplantatie (BEAM)
- 3x DHAP (liever BV-DHAP dan DHAP maar vergoedingsstatus onduidelijk)
- CT na kuur 2, indien geen PR over op tweedelijns therapie
- PET-CT na kuur 3, indien geen mCR over op tweedelijns therapie
- brentuximab
- aantal kuren: mCR +2
- 3x DHAP (liever BV-DHAP dan DHAP maar vergoedingsstatus onduidelijk)
- <65-70 en fit genoeg voor autologe stamceltransplantatie (BEAM)
- indien RT mogelijk is
- ook monotherapie radiotherapie kan curatief zijn
- met name bij vroeg stadium ziekte
- incurabel
- CD30-positief: brentuximab
- na AuSCT of 2 eerdere therapieen, indien geen AuSCT dus eerst conventionele chemotherapie
- lange termijn PFS: curve (Chen et al)
- matige CD30-kleuring geen reden voor geen therapie (Van der Weyden, Blood Cancer Journal, 2017), ook geen exclusiecriterium in originele studie Younes, JCO, 2012
- na brentuximab: nivolumab (AMC)
- RR 65-70%, CR 9-22%, PFS 8-17 m Younes et al., Armand, Checkmate 205, Chen, Keynote-087
- 40% in Checkmate 205 nog behandeling na 18 maanden (voorbij standaard criteria van progressieve ziekte)
- RR 65-70%, CR 9-22%, PFS 8-17 m Younes et al., Armand, Checkmate 205, Chen, Keynote-087
- chemotherapische opties
- 3x DHAP / VIM
- IGEV
- ChlVVP
- CD30-positief: brentuximab
{kind=link}
3 prognose
3.1 getallen
3.1.1 vroeg stadium
- HD14 OS-5jr 4x ABVD 97% (en HD10 94%)
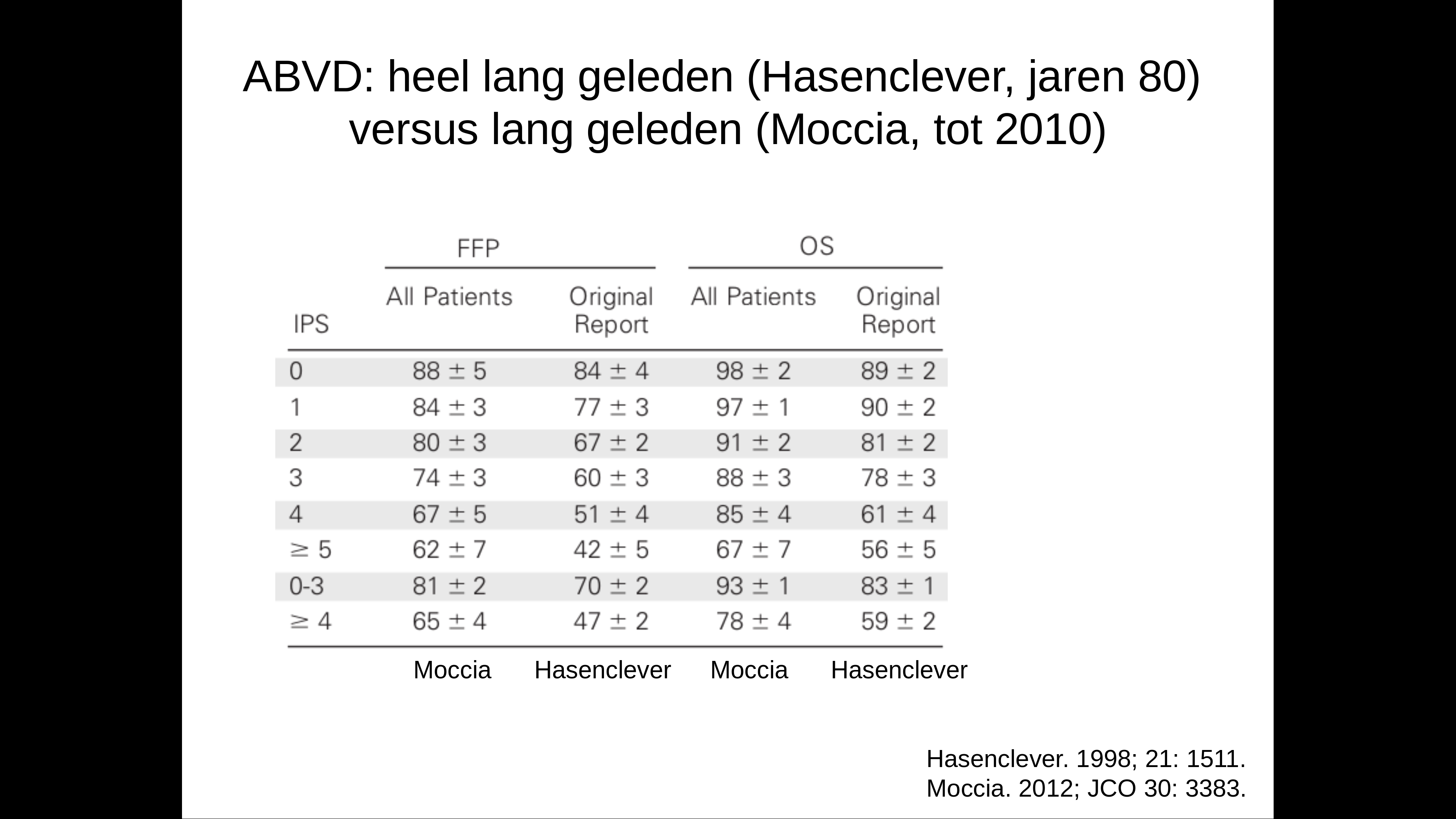
3.1.2 gevorderd
- IPS - Hasenclever: curve
- Serum albumin <4 g/dL
- Hemoglobin <10.5 g/dL
- Male gender
- Age >45 years
- Stage IV disease
- White blood cell count ≥15,000/microL
- Absolute lymphocyte count <600/microL and/or <8 percent of the total white blood cell count
{kind=link}
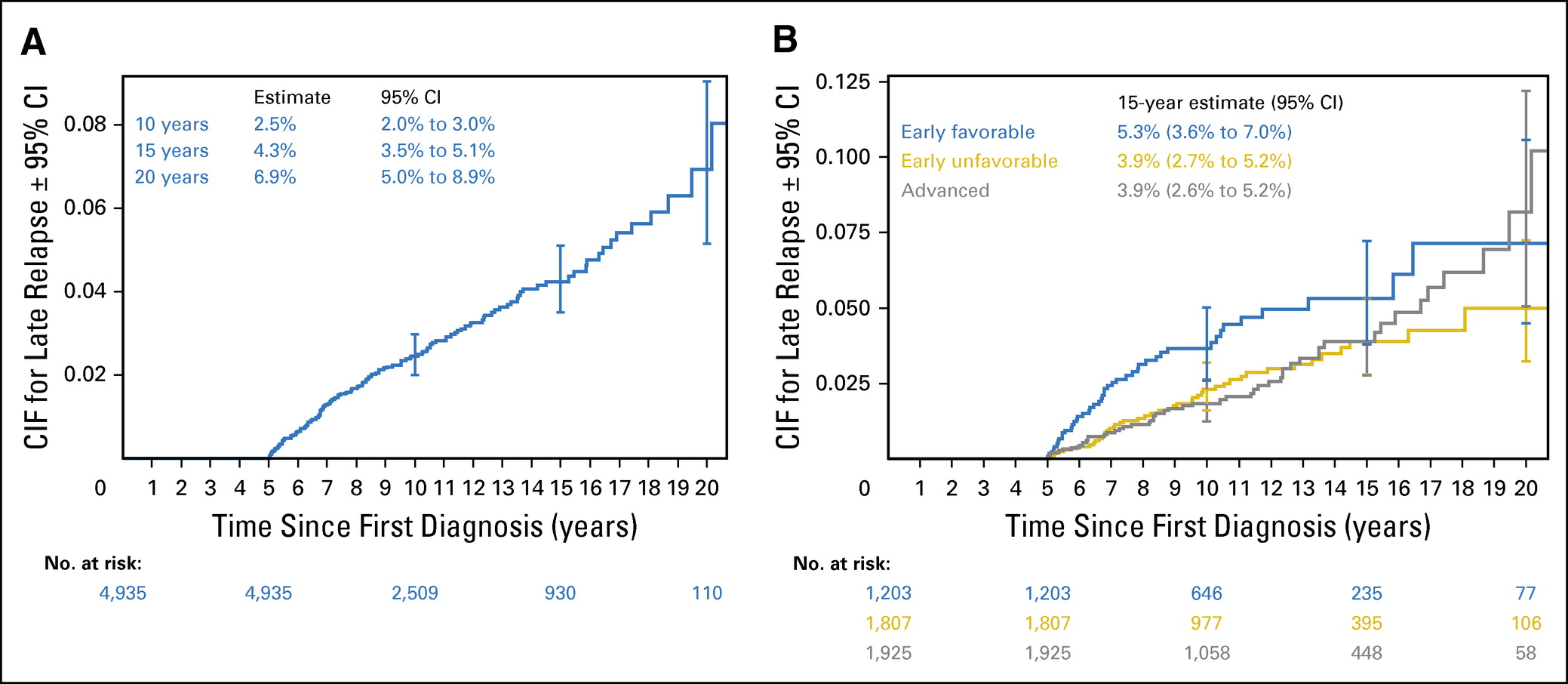
3.2 timing recidief
- tot 20 jaar na initiele diagnose (Brockelmann, JCO, 2017: curve)
{kind=link}
4 Ann-Arbor-classificatie2
- Stage I: single lymph node region or lymphoid structure (as spleen, thymus and Waldeyer's ring)
- Stage II
- two or more lymph node regions or structures on same side of diaphragm
- hilar nodes should be considered to be "lateralized"
- number of anatomical regions should be indicated by a subscript (e.g. II3)
- Stage III: lymphoid structures on both sides of the diaphragm
- III1: spleen or splenic, hilar, coeliac or portal node involvement
- III2: paraaortic, iliac or mesenteric node involvement
- thus, also supradiaphragmatic disease with splenomegaly
- Stage IV: extensive extranodal disease
- B: unexplained weight loss >10% body weight during 6 months, unexplained fever above 38°C during the previous month, drenching night sweats during the previous months
- S: spleen
- X / bulky: largest dimension (cm) >10 or mediastinal: maximum width is equal or greater than one-third of the internal transverse diameter of the thorax at the T5-T6 level maximal inspiration in the upright position at a source-skin distance of 2 m
- involvement of extra lymphatic tissue on one side of the diaphragm by limited direct extension from an adjacent nodal site
- prognosis equivalent to that for nodal disease
- multiple extranodal deposits: stage IV
- single extralymphatic site as only site of disease: IE
5 GHSG-risicoclassificatie
- indien 1 van de volgende aanwezig aanwezig: "intermediate stage" (en dus geen early stage)
- Large mediastinal mass, size at least one third of the maximum thorax diameter
- extra-nodale ziekte
- >2 klierstations
- verhoogd BSE
- > 50 mm/h bij IA, IIA, en
- > 30 mm/h bij IB,IIB
6 EORTC-risicoclassificatie
- indien 1 van de volgende aanwezig: unfavorable
- >50 jaar
- large mediastinal adenopathy (>=0,35 MT ratio: op Th5 ratio tumor/thorax diameter op staande X-thorax)
- bij BSE => 50/h B-symptomen
- bij BSE => 30 mm/h B symptomen
- >3 klierstations
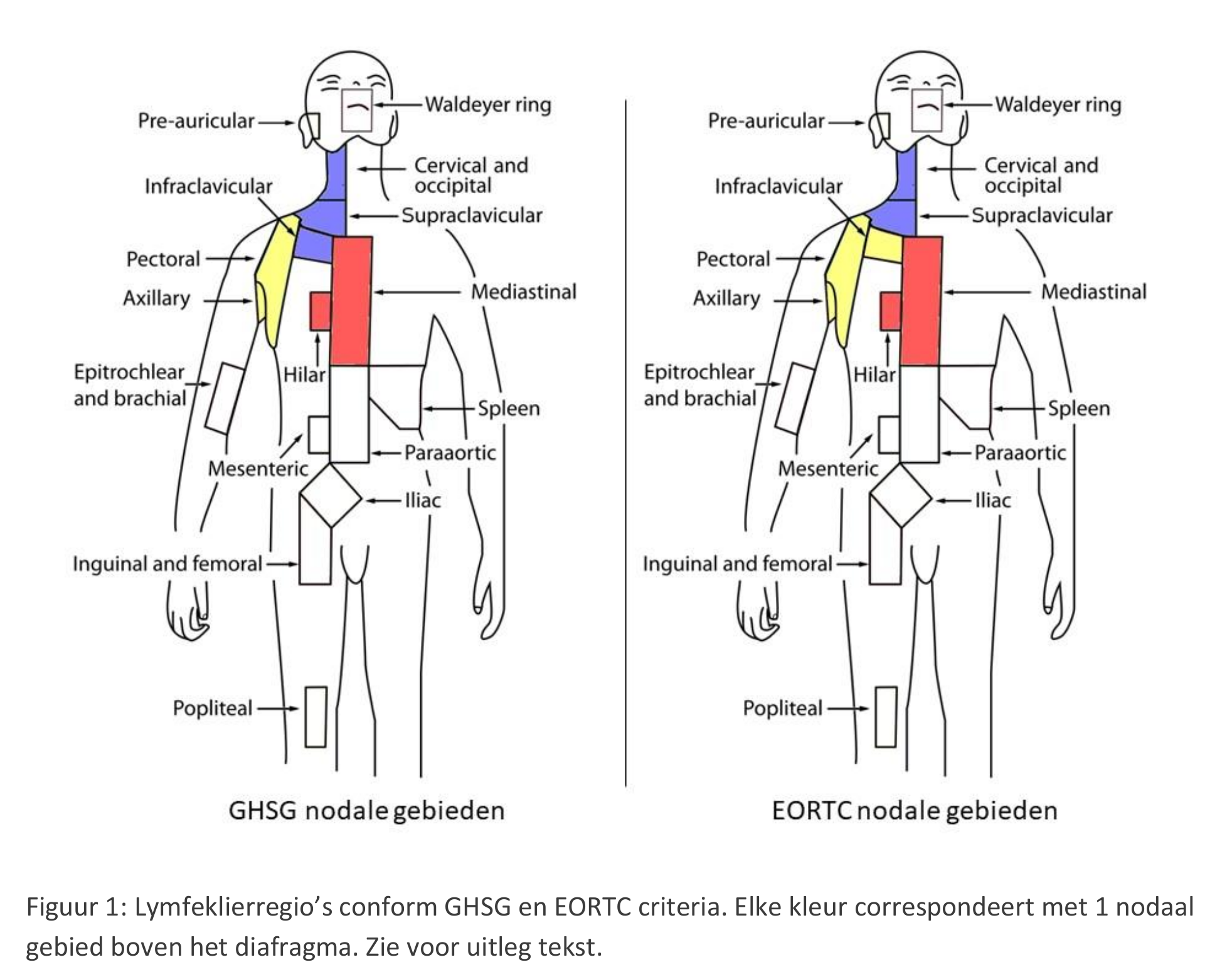
7 Klierstations
- supraclaviculaire klierstations volgens EORTC en GSHG grafisch weergegeven
- klierstations volgens EORTC supraclaviculair uitgeschreven
- infradiafragmale klierstations EORTC nog uitzoeken
{kind=link}
7.1 GSHG uitgeschreven
- Area A: right cervical + right infra-/supra-clavicular/nuchal lymph nodes
- Area B: left cervical + right infra-/supra-clavicular/nuchal lymph nodes
- Area C: right/left hilar + mediastinal lymph nodes
- Area D: right axillary lymph nodes
- Area E: left axillary lymph nodes
- Area F: lymph nodes of the upper abdomen (spleen hilum, liver hilum, coeliacal)
- Area G: lymph nodes of the lower abdomen (spleen hilum, liver hilum, coeliacal)
- Area H: right iliac lymph nodes
- Area I: left iliac lymph nodes
- Area K: right inguinal + femoral lymph nodes
- Area L: left inguinal + femoral lymph nodes
8 voetnoten
Voetnoten:
1
- prognose slechter door associatie met slechtere prognostische factoren
- maar geen reden om van radiotherapie af te zien
- https://www.sciencedirect.com/science/article/pii/S0167814003000549?via=ihub
- Iannitto, Haematologica, 1997
2
- Carbone PP, Kaplan HS, Musshoff K, et al. Report of the committee on Hodgkin's disease staging classification. Cancer. Res. 31:1860-1861, 1971.
- Lister TA, Crowther D, Sutcliffe SB, et al. Staging for Hodgkin's disease. Report of a committee convened to discuss the evaluation and staging of patients with Hodgkin's disease: Cotswolds meeting. J. Clin. Oncol. 7:1630-1636, 1989 (Erratum J. Clin. Oncol. 8:1602, 1990).