Hodgkinlymfoom (HL)
Inhoudsopgave
Terug naar beginpagina de-heer.eu.
Terug naar overzicht hematologische diagnosen http://de-heer.eu
1 onderzoek
- PET-CT (indien evt. vroeg-stadium mogelijk: in stralingshouding)
- geen beenmergonderzoek
- Ann-Arbor-classificatie (let op: stadium II-B + bulky = gevorderd HL)
- vroeg-stadium:
- consult radiotherapie voor start chemotherapie
- GHSG-risicoclassificatie
- EORTC-risicoclassificatie
- consult radiotherapie voor start chemotherapie
- overweeg ook bij vroeg stadium vruchtbare vrouw te verwijzen naar de fertiliteitpoli
- semenpreservatie
- altijd MDO:
- vroeg-stadium: afweging lange termijneffecten RT versus gering inferieure therapie zonder radiotherapie
- bij twijfel proefplanning overwegen
- indicaties weglaten radiotherapie
- altijd: <35 jaar en mammae in veld (bv. mediastinaal en bilateraal axillair)
- te overwegen:
- bulky mediastinaal, mediastinaal en 1 klier in oksel
- proximaal in hals
- bulky mediastinaal, mediastinaal en 1 klier in oksel
- altijd: <35 jaar en mammae in veld (bv. mediastinaal en bilateraal axillair)
- bij twijfel proefplanning overwegen
- gevorderd stadium
- >70 of >60 en niet fit: CHOP
- >60 en fit: ABVD
- <60 keuze maken tussen ABVD of BEACOPP
- argumenten voor escBEACOPP: stadium IV, hoge tumorload (tumor >7 cm), IPS >1, voorkeur patient (korter schema, betere PFS-5j 82% vs 92% (OS 95% vs 98%)
- argumenten voor ABVD: fertiliteit, mogelijk meer lange termijneffecten (secundaire maligniteiten, MDS), PS >2 boven 40 of co-morbiditeit
- argumenten voor escBEACOPP: stadium IV, hoge tumorload (tumor >7 cm), IPS >1, voorkeur patient (korter schema, betere PFS-5j 82% vs 92% (OS 95% vs 98%)
- >70 of >60 en niet fit: CHOP
- vroeg-stadium: afweging lange termijneffecten RT versus gering inferieure therapie zonder radiotherapie
2 therapie
Bij zwangeren, overweeg https://www.ab-cip.org/ en zie ref
Let op! in escBEACOPP zit nu dacarbazine en dexamethason: BEACODDac.
2.1 therapie eerste lijn
2.1.1 esc BEACOPP versus ABVD
- esc BEACOPP geniet voorkeur boven ABVD tenzij IPS 0-1, dan ook ABVD te overwegen
- geen esc BEACOPP bij: >60 jaar, >50 jaar en ECOG 1, contra-indicatie bleo, fertiliteitsoverwegingen
- BV-AVD is de voorkeur van behandeling bij gevorderd stadium III/IV HL bij contra-indicatie esc BEACOPP
2.1.2 interim-PET/CT
- op dag 23-25 van kuur 2
- indien behandeling met ABVD gestart wordt:
- mCR: bleomycine mag weggelaten worden bij vervolg behandeling
- geen mCR:
- over op escBEACOPP
- indien conditie geen escalatie naar escBEACOPP toestaat toch PET-CT maken omdat weglaten bleomycine na kuur 2 alleen veilig gebleken is bij mCR
- alternatief bij geen mCR (of CT zonder PET): continueren bleomycine onder scherpe controle LF (niet gevalideerd beleid)
- over op escBEACOPP
- mCR: bleomycine mag weggelaten worden bij vervolg behandeling
- indien behandeling met escBEACOPP gestart wordt:
- al dan geen mCR bepaalt aantal kuren escBEACOPP dat nog volgt
- al dan geen mCR bepaalt aantal kuren escBEACOPP dat nog volgt
2.1.3 vroeg stadium
- infradiafragmaal lymfoom is geen reden om af te wijken van protocol[1]
- schema met radiotherapie
- >70 of >60 en niet fit: 3x CHOP-21 + IN-RT
- ABVD-bevattend schema
- EORTC/GHSG favourable: 2x ABVD + 20 Gy INRT (op dag 21 na laatste gift)
- GHSG unfavourable
- EORTC favourable: 3x A(B)VD + 20 Gy INRT
- EORTC unfavourable: 4x A(B)VD + 30 Gy INRT
- EORTC favourable: 3x A(B)VD + 20 Gy INRT
- interim-CT geen mCR: over op 2x escBEACOPP
- EORTC/GHSG favourable: 2x ABVD + 20 Gy INRT (op dag 21 na laatste gift)
- >70 of >60 en niet fit: 3x CHOP-21 + IN-RT
- schema zonder radiotherapie
- non-bulky: 4x A(B)VD
- bulky: 6x A(B)VD
- non-bulky: 4x A(B)VD
- evaluatie na therapie
2.1.4 gevorderd
- COBRA-studie (zie studieoverzicht)
- CHOP: 6x CHOP-21
- ABVD: 2x ABVD
- D1-3: nog 4x AVD
- D4-5: 4x escBEACOPP
- D1-3: nog 4x AVD
- escBEACOPP: 2x escBEACOPP
- D1-3: 2x escBEACOPP
- D4-5: 4x escBEACOPP
- D1-3: 2x escBEACOPP
- evaluatie na therapie
2.1.5 eindevaluatie
- in bestralingspositie bij grote kans op aanvullende radiotherapie
- na chemoradiotherapie
- na 3 maanden
- niet nodig bij beperkt stadium en negatieve interim/plannings-PET-CT
- na 3 maanden
- na behandelplan zonder radiotherapie
- na 4-6 weken
- indien nieuwe lesies of groei na eerdere afname, en <65 tot 70
- PA-bevestiging: tweedelijns therapie
- geen PA-bevestiging mogelijk: na 2 maanden PET-CT herhalen
- PA-bevestiging: tweedelijns therapie
- indien "nog resterende FDG-avide afwijkingen" >1,5 cm: aanvullende RT, 36 Gy op FDG-avide afwijkingen
- na 4-6 weken
2.2 recidief
- curatieve intentie
- <65-70 en fit genoeg voor autologe stamceltransplantatie (BEAM)
- 3x DHAP
- overweeg toevoegen brentuximab bij recidief binnen 1 jaar: BV-DHAP (Hagenbeek, Haematologica, 2019)
- CT na kuur 2, indien geen PR over op tweedelijns therapie
- PET-CT na kuur 3, indien geen mCR over op tweedelijns therapie, bv.
- brentuximab (aantal kuren: mCR +2)
- brentuximab (aantal kuren: mCR +2)
- bij hoog-risico is onderhoud brentuximab na AuSCT een vergoede overweging (indicatie nog niet uitgekristalliseerd)
- overweeg toevoegen brentuximab bij recidief binnen 1 jaar: BV-DHAP (Hagenbeek, Haematologica, 2019)
- bij nierfunctiestoornis door DHAP
- reversibel: (BV-)DHAC
- niet-reversibel: (BV-)ICE of (BV-)IGEV (Abuelgasim, BMT, 2019)
- reversibel: (BV-)DHAC
- 3x DHAP
- <65-70 en fit genoeg voor autologe stamceltransplantatie (BEAM)
- indien RT mogelijk is
- ook monotherapie radiotherapie kan curatief zijn
- met name bij vroeg stadium ziekte
- ook monotherapie radiotherapie kan curatief zijn
- incurabel
- CD30-positief: brentuximab
- registratie: na AuSCT of 2 eerdere therapieen, dus indien geen AuSCT verricht dus eerst conventionele chemotherapie
- curve PFS (Chen et al)
- matige CD30-kleuring
- geen reden om af te zien van brentuximab (Van der Weyden, Blood Cancer Journal, 2017)
- ook geen exclusiecriterium in originele studie Younes, JCO, 2012
- geen reden om af te zien van brentuximab (Van der Weyden, Blood Cancer Journal, 2017)
- registratie: na AuSCT of 2 eerdere therapieen, dus indien geen AuSCT verricht dus eerst conventionele chemotherapie
- na brentuximab: ICI (AMC)
- RR 65-70%, CR 9-22%, PFS 8-17 m Younes et al., Armand, Checkmate 205, Chen, Keynote-087
- 40% in Checkmate 205 nog behandeling na 18 maanden (geen standaard criteria voor PD)
- RR 65-70%, CR 9-22%, PFS 8-17 m Younes et al., Armand, Checkmate 205, Chen, Keynote-087
- chemotherapische opties
- 6x DHAP (of 3x DHAP/VIM)
- IGEV
- ChlVVP
- 6x DHAP (of 3x DHAP/VIM)
- CD30-positief: brentuximab
{kind=link}
2.3 NLPHD
- stadium I: hoge dosis RT
- stadium II: hoge dosis RT, evt voorafgegaan door 2x ABVD [3]
- stadium III/IV: wait-and-see bij geen klachten
2.4 follow-up
- 1e jaar a 3 maanden
- 2e jaar a 4 maanden
- 3e tot 5e jaar a 6 maanden
3 prognose
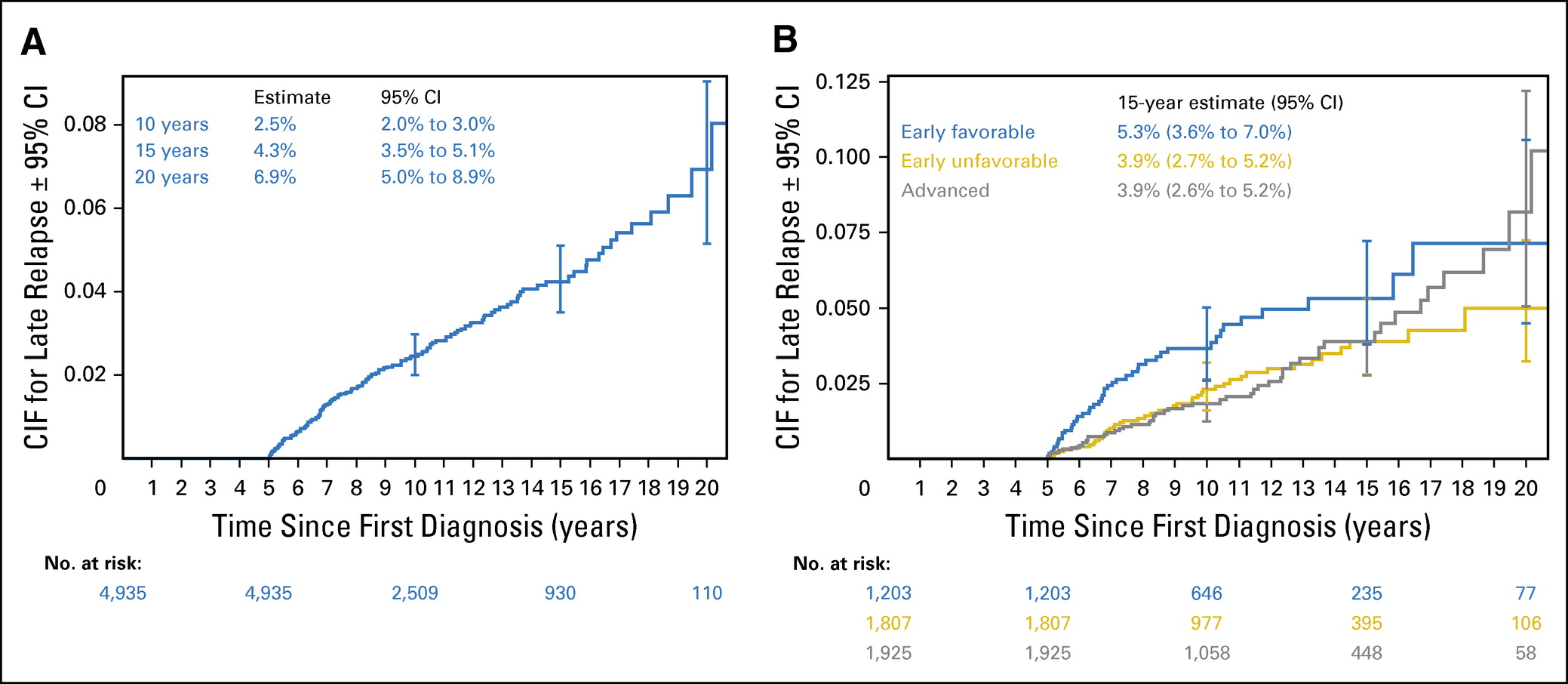
- vroeg stadium
- OS-5jr na 4x ABVD 97% in HD14 en 94% in HD10
- tot 20 jaar na initiele diagnose is recidief mogelijk (Brockelmann, JCO, 2017: curve)
- OS-5jr na 4x ABVD 97% in HD14 en 94% in HD10
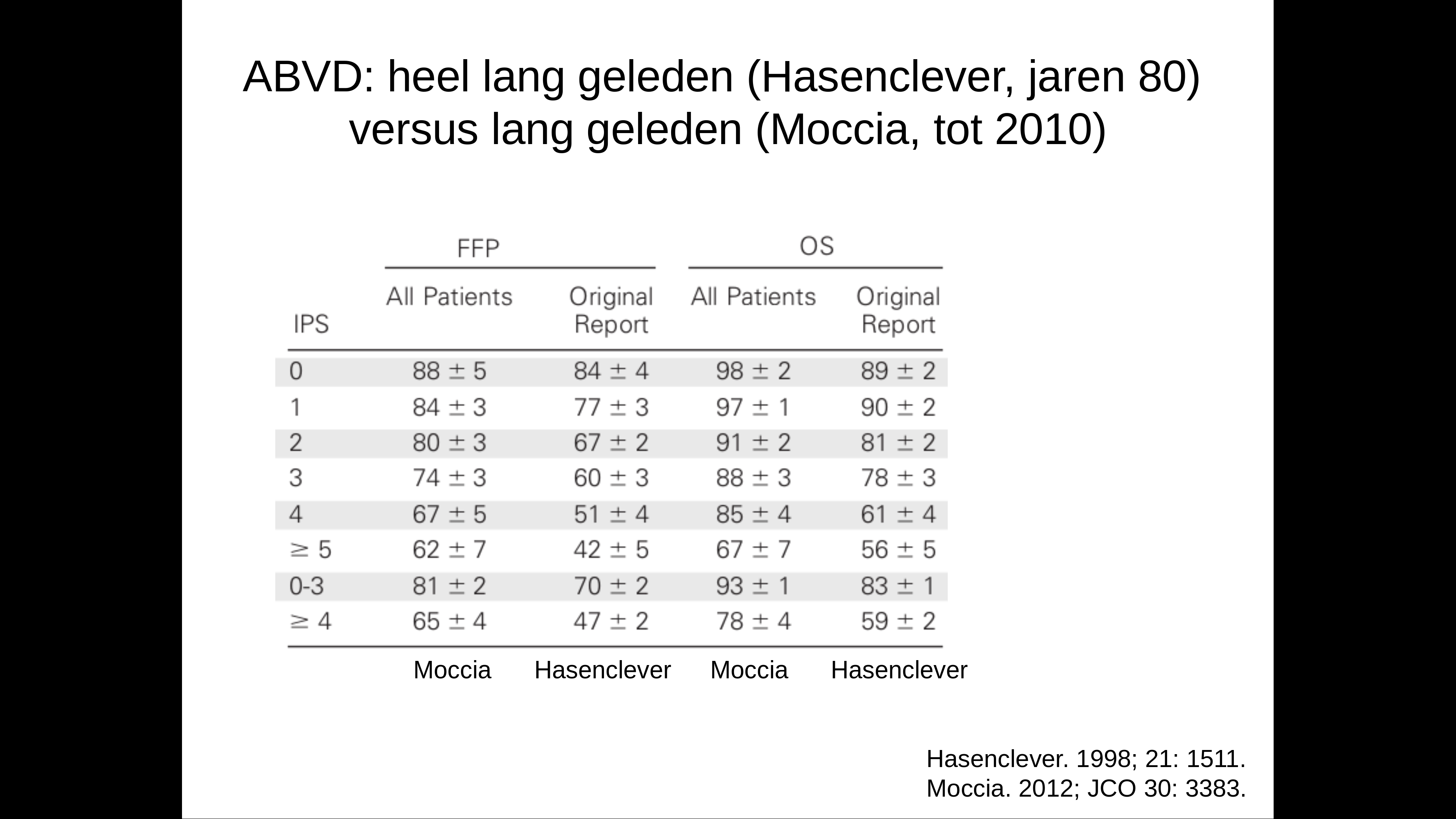
- gevorderd
- curve volgens Hasenclever
- ABVD versus BEACOPP: verschil in PFS 5 tot 15%, verschil in OS mogelijk 2,5%
- curve volgens Hasenclever
{kind=link}
{kind=link}
4 GHSG
- 1 van de volgende aanwezig aanwezig = "intermediate stage" (anders early stage)
- large mediastinal mass, size at least one third of the maximum thorax diameter
- extra-nodale ziekte
- >2 klierstations
- verhoogd BSE
- > 50 mm/h bij IA, IIA, en
- > 30 mm/h bij IB,IIB
- > 50 mm/h bij IA, IIA, en
- large mediastinal mass, size at least one third of the maximum thorax diameter
5 EORTC
- 1 van de volgende aanwezig = unfavorable
- >50 jaar
- large mediastinal adenopathy (>=0,35 MT ratio: op Th5 ratio tumor/thorax diameter op staande X-thorax)
- bij BSE => 50/h bij geen B-symptomen
- bij BSE => 30 mm/h bij B-symptomen
- >3 klierstations
- >50 jaar
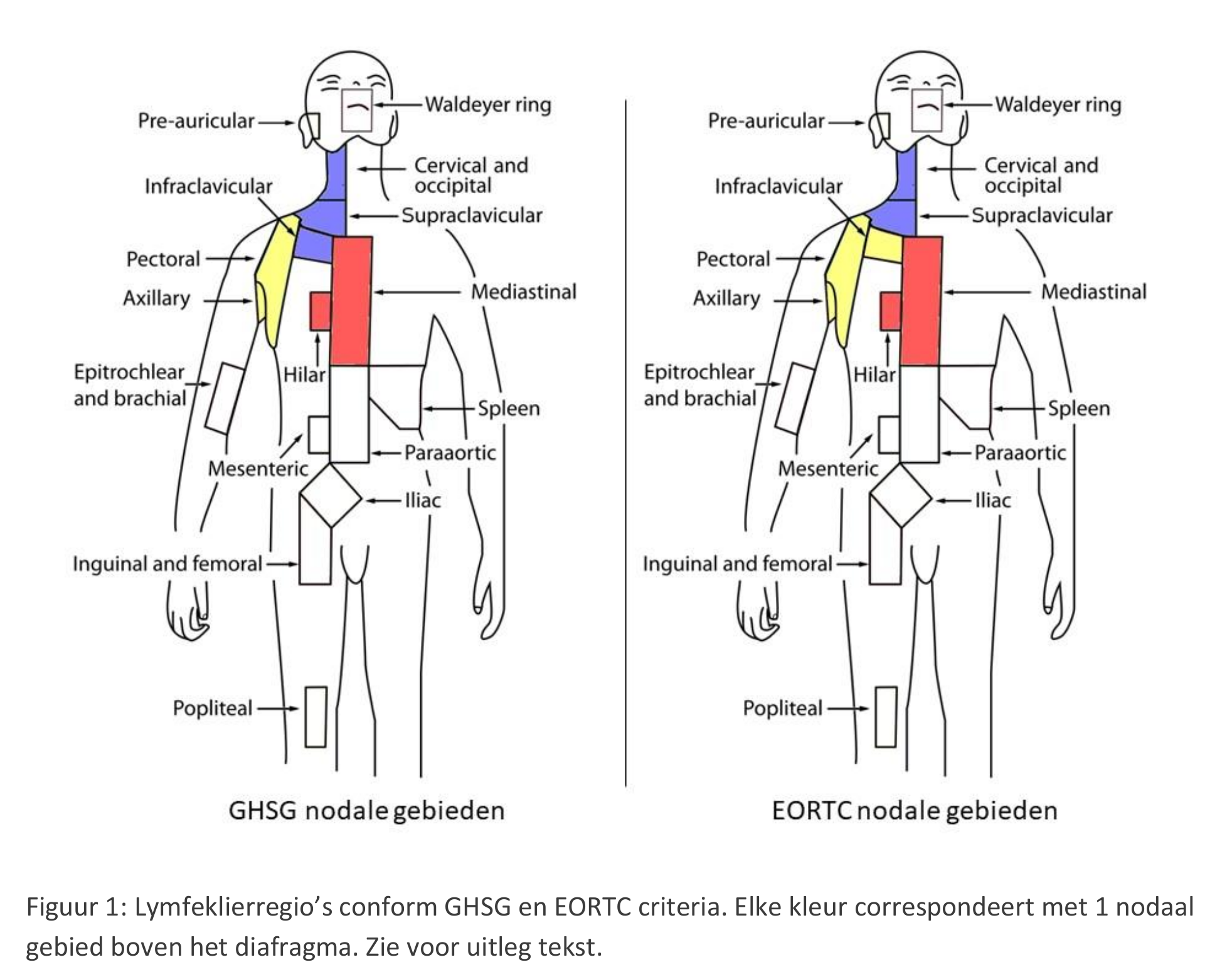
6 Klierstations
{kind=link}
6.1 GSHG uitgeschreven
- Area A: right cervical + right infra-/supra-clavicular/nuchal lymph nodes
- Area B: left cervical + right infra-/supra-clavicular/nuchal lymph nodes
- Area C: right/left hilar + mediastinal lymph nodes
- Area D: right axillary lymph nodes
- Area E: left axillary lymph nodes
- Area F: lymph nodes of the upper abdomen (spleen hilum, liver hilum, coeliacal)
- Area G: lymph nodes of the lower abdomen (spleen hilum, liver hilum, coeliacal)
- Area H: right iliac lymph nodes
- Area I: left iliac lymph nodes
- Area K: right inguinal + femoral lymph nodes
- Area L: left inguinal + femoral lymph nodes
7 Hasenclever
| Serum albumin <4 g/dL |
| Hemoglobin <10.5 g/dL |
| Male gender |
| Age >45 years |
| Stage IV disease |
| White blood cell count ≥15,000/microL |
| Absolute lymphocyte count <600/microL and/or <8 percent of the total white blood cell count |
8 Ann-Arbor-classificatie[2]
- Stage I: single lymph node region or lymphoid structure (as spleen, thymus and Waldeyer's ring)
- Stage II
- two or more lymph node regions or structures on same side of diaphragm
- hilar nodes should be considered to be "lateralized"
- number of anatomical regions should be indicated by a subscript (e.g. II3)
- two or more lymph node regions or structures on same side of diaphragm
- Stage III: lymphoid structures on both sides of the diaphragm
- III1: spleen or splenic, hilar, coeliac or portal node involvement
- III2: paraaortic, iliac or mesenteric node involvement
- thus, also supradiaphragmatic disease with splenomegaly
- III1: spleen or splenic, hilar, coeliac or portal node involvement
- Stage IV: extensive extranodal disease
- B: unexplained weight loss >10% body weight during 6 months, unexplained fever above 38°C during the previous month, drenching night sweats during the previous months
- S: spleen
- X / bulky: largest dimension (cm) >10 or mediastinal: maximum width is equal or greater than one-third of the internal transverse diameter of the thorax at the T5-T6 level maximal inspiration in the upright position at a source-skin distance of 2 m
- involvement of extra lymphatic tissue on one side of the diaphragm by limited direct extension from an adjacent nodal site
- prognosis equivalent to that for nodal disease
- multiple extranodal deposits: stage IV
- single extralymphatic site as only site of disease: IE
- prognosis equivalent to that for nodal disease
10 brief
Een nodulair paragranuloom, oftewel de niet klassieke vorm van de ziekte van Hogdkin, gedraagt zich anders dan een klassiek Hogdkin lymfoom. Het kan beschouwd worden als een B-cel NHL van lage maligniteitsgraad. Bij beperkte ziekte (AA stadium I) word het klierpakket in opzet curatief bestraald. De ziekte kan recidiveren, waarbij in geval van uitgebreidere ziekte behandeld kan worden met chemotherapie. De levensverwachting bij stadium I benaderd die van de gezonde bevolking, hoewel ook transformatie op kan treden naar aggresievere varianten van het Non-Hodgkin lymfoom. Ik blijf patiënt de komende 5 jaar met intervallen van 4-6 maanden vervolgen.
11 voetnoten
[1]
- prognose slechter door associatie met slechtere prognostische factoren
- maar geen reden om van radiotherapie af te zien
- https://www.sciencedirect.com/science/article/pii/S0167814003000549?via%3Dihub
- Iannitto, Haematologica, 1997
[2]
- Carbone PP, Kaplan HS, Musshoff K, et al. Report of the committee on Hodgkin's disease staging classification. Cancer. Res. 31:1860-1861, 1971.
- Lister TA, Crowther D, Sutcliffe SB, et al. Staging for Hodgkin's disease. Report of a committee convened to discuss the evaluation and staging of patients with Hodgkin's disease: Cotswolds meeting. J. Clin. Oncol. 7:1630-1636, 1989 (Erratum J. Clin. Oncol. 8:1602, 1990).
[3]
- How I treat, Hoppe: http://www.bloodjournal.org/content/122/26/4182
- ESMO, Eichenauer: https://www.esmo.org/Guidelines/Haematological-Malignancies/Hodgkin-Lymphoma
- NCCN http://williams.medicine.wisc.edu/hodgkins.pdf
- GHSG, https://www.onlinelibrary.wiley.com/doi/full/10.1002/hon.2067
- ILROG, https://www.ncbi.nlm.nih.gov/pubmed/23790512 mmm
- How I treat, Spinner, 2018 BJH: https://onlinelibrary.wiley.com/doi/full/10.1111/bjh.15616
- Savage et al.