T-cellymfoom
Inhoudsopgave
Terug naar beginpagina de-heer.eu.
Zie de aparte pagina voor het extranodaal NK/T-cellymfoom.
1 Verplicht onderzoek
- standaard lab
- PET-CT
- beenmergonderzoek
- enige verdenking ATLL: HTLV-serologie
- afhankelijk van PA-diagnose:
| EBV-geassocieerd lymfoom | PCR EBV |
| dunne darmtumor / EATL | coeliakie? |
| hepatosplenisch γδ-lymfoom | Crohn/infliximab of immuunsuppressie? |
2 Therapie
2.1 Algemeen
- er zijn vele varianten T-cellymfoom, in volgorde van frequentie van voorkomen:
- Peripheral T cell lymphoma, not otherwise specified (NOS)
- Anaplastic large cell lymphoma, primary systemic type
- Angioimmunoblastic T cell lymphoma
- Extranodal NK/T cell lymphoma, nasal type (ENKL)
- Subcutaneous panniculitis-like T cell lymphoma
- Enteropathy associated T cell lymphoma
- Hepatosplenic T cell lymphoma
- ATLL
- Peripheral T cell lymphoma, not otherwise specified (NOS)
- let op
- verminderde cellulaire afweer: cotrimoxazol/valaciclovir bij chemotherapie
- zeldzame complicatie van T-NHL is HLH
- verminderde cellulaire afweer: cotrimoxazol/valaciclovir bij chemotherapie
2.2 PTCL nno
2.2.1 Eerste lijn
- T-cellymfoom van de huid waaronder ook αβ panniculitis-like lymphoma
- ATLL
- zidovudine plus interferon-alfa
- CHOEP gevolgd door allo-SCT
- zidovudine plus interferon-alfa
- EBV-positief en laag stadium AITL: monotherapie rituximab te overwegen?
- anders
- stadium I
- <65 jaar: 3x CHOEP-21 waarna RT
- >65 jaar: 2x CHOP-21 waarna RT
- <65 jaar: 3x CHOEP-21 waarna RT
- stadium II-IV
- ab panniculitis-like TCL: prednison
- ALCL
- Alk-negatief
- fit: 6x CHOP + BEAM
- unfit: 6x BV-CHP (of 6x CHOP)
- fit: 6x CHOP + BEAM
- Alk-positief
- fit: 6x CHOEP (of 6x BV-CHP)
- unfit: 6x BV-CHP (of 6x CHOP)
- tolerantie >65 voor CHOEP beduidend lager: https://www.annalsofoncology.org/action/showPdf?pii=S0923-7534%2819%2963550-7
- fit: 6x CHOEP (of 6x BV-CHP)
- Alk-negatief
- <65 jaar: 6x CHOP-14 en ASCT
- >65 jaar: 6x CHOP-21 met Neulasta, indien veel toxiciteit: deescalatie, indien goede respons en tolerantie alsnog ASCT overwegen
- ab panniculitis-like TCL: prednison
- stadium I
- specifieke aanvullende overwegingen afhankelijk van subtype
- EATL
- vaak chirurgische debulking nodig om behandeling mogelijk te maken
- overweeg volgens bemoedigende kleine studie: 1 CHOP-kuur, 6x ifosfamide/epirubicine/etoposide en HD-MTX, daarna: BEAM (Sieniawski, Blood, 2010: 5-jaar OS 50-60%)
- vaak chirurgische debulking nodig om behandeling mogelijk te maken
- hepatosplenisch γδ-lymfoom: overweeg volgens bemoedigende kleine studie DHAP gevolgd door BEAM (Foppoli, EJH, 2014)
- TFH / AITL
- bij EBV-positief AITL rituximab vaak toegevoegd aan chemotherapie
- echter slechts een studie met rituximab verricht: geen effect
- ter overweging, EBV-positief en laag stadium: monotherapie rituximab?
- echter slechts een studie met rituximab verricht: geen effect
- PET-CT voor autologe stamceltransplantatie
- bij EBV-positief AITL rituximab vaak toegevoegd aan chemotherapie
- BI-ALCL
- EATL
2.2.2 Recidief
- nog geen AuSCT en <65-70
- chemo-refractair (relapse <12 maanden) en indien CD30-positief: 6x brentuximab, 80% respons (langdurige remissies, ook zonder consolidatie)
- chemo-sensitief of CD30-negatief: DHAP/GDP + BEAM als bij DGBCL zonder R, kans op CR laag maar niet nul
- chemo-refractair (relapse <12 maanden) en indien CD30-positief: 6x brentuximab, 80% respons (langdurige remissies, ook zonder consolidatie)
- reeds AuSCT en voldoende fit en CR: na inductie (en evt. bridging bij PR) opwerken voor allogene SCT[4]
- alternatief indien CD30-positief
- ALCL: 6x brentuximab, 80% respons
- ander T-NHL (soms PTCL, 50% EATL, AITL): brentuximab niet geregistreerd maar te overwegen
- ALCL: 6x brentuximab, 80% respons
- alternatief indien CD30-positief
- derde lijn, en bij respons alsnog SCT overwegen:
- NIVEAU-studie
- DHAP / IGEV
- CDK9-studie
- AITL
- zie tabel Moskovitz[1]
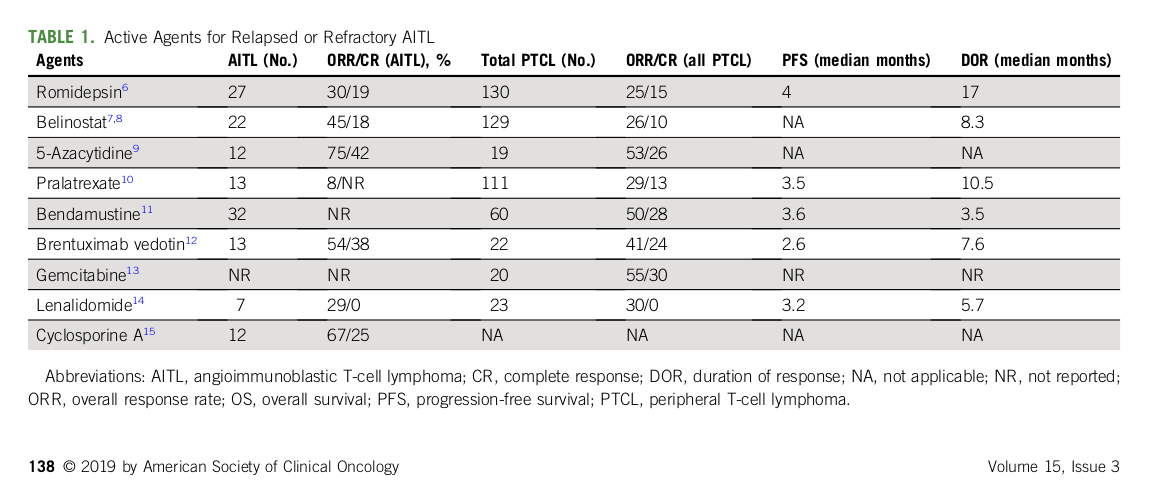
- MTX 15 mg 1x/week (alternatief pralatrexaat) en 1dd 50 mg prednison waarna afbouwschema
- zie tabel Moskovitz[1]
- NIVEAU-studie
3 Prognose
3.1 PTCL-NOS
- 10% overlijdt binnen paar maanden, 10% leeft na 10 jaar [2]
3.2 ACLC
- Alk-: 10% overlijdt binnen paar maanden, 10-30% leeft na 10 jaar[3]
- Alk+: 60% leeft na 10 jaar
3.3 EATL
- 5-jaar OS 8-20%
3.4 AITL
- 64% CR met CHOP
- OS
- mediaan 18 maanden
- AuSCT lijkt prognose te verbeteren
- allo kan curatief zijn in selecte subgroep
- long term survival: bij ongeveer derde
- Int Periph T-c Lymphoma Project: 243 patients, 5 jaar OS 33% en PFS 18%
- Japan: 207 patients, 3 jaar OS 54%, PFS 38%
- Int Periph T-c Lymphoma Project: 243 patients, 5 jaar OS 33% en PFS 18%
- mediaan 18 maanden
- complicaties
- overlijden vaak door infecties
- kan soms overgaan in agressief B-cellymfoom (door mutatie in EBV-positieve B-celkloon die vaak ook gevonden wordt)
- overlijden vaak door infecties
4 Onderscheid
| Entity | Positief | Vaak | Soms | Negatief |
|---|---|---|---|---|
| AITL | CD3 and CD4 | TCR genes rearranged | BCL-6, CD10, verlies pan-T, EBV/HHV-6 in reactieve cells | |
| EATL | klonaal TCR | CD3, mp 9q34, coeliakie HLA haplotype | CD8-, CD30 | CD4 |
| ENKL | CD2, cCD3, CD56, cytotoxic, EBER | TCR germline | sCD3 | |
| Hepatosplenic | CD2/7/16, sCD3, g/d TCR of a/b TCR | CD56, isochrome 7q | CD4, CD5, CD8. | |
| Panniculitis-like | CD3, CD8, a/b TCR, cytotoxisch, klonale TCR | CD2/5/7 | CD4, CD56, TCR g | |
| ALCL | CD30 | >-1 pan-T, Alk | ||
| PTCL nos | one or more pan-T antigens | verlies pan-T | ||
| NK cell enteropathy | CD7, cCD3, TIA-1 and/or Granzyme B, lage MIB | EBV, CD4/5/8/10/20/30/138/68, PAX-5, TCR klonaliteit | ||
- cytotoxic granule proteins: granzyme B or perforin
- pan-t: CD2/3/5/7
5 Referenties
- How I Treat: Moskowitz et al.
- ESMO guidelines 2015
6 Voetnoten
[1] - referenties
- 4. Coiffier, JCO, 30:631-636, 2012.
- 5. Horwitz, Hematol Oncol 31:147, 2013.
- 6. O’Connor, JCO, 33:2492-2499, 2015.
- 7. Delarue, Blood, 128:4164, 2016.
- 8. O’Connor, JCO, 29:1182-1189, 2011.
- 9. Damaj, JCO, 31:104-110, 2013.
- 10. Horwitz, Blood, 123:3095-3100, 2014
- 11. Zinzani, Ann Oncol 21:860-863, 2010.
- 12. Dueck, Cancer 116:4541-4548, 2010.
- 13. Advani, Leuk Lymphoma 48:521-525, 2007/
[2] Weisenberger, 2011 - n=340
[3] Savage, 2008, n=159 systemisch, 55% Alk+ en 45% Alk0
[4] EBMT 2009 waarde allo
[5] - referenties
- zie Vose et al.
- Kim SJ, Lancet Oncol 2016
- Yang Y, Blood 2015
- PINK-E score
[6] etoposide geeft een 20% toename van de 3-jaar EFS in jongere patienten, maar niet bij oudere patienten. OS is niet significant verschillend. Een beperking is dat het aantal oudere patienten bij wie dit onderzocht is te klein is om zekere uitspraken te doen. Derhalve valt etoposide te overwegen bij fitte patienten >65 jaar